Macrophages are immune system cells that normally eat invading foreign microbes and digest them. However, microbiologists have discovered that certain microbes have evolved ways to invade macrophages, to take over their cellular machinery, to form colonies inside the macrophages, and to slowly replicate themselves and form new colonies.
Macrophage colonies are an important causal factor in
Rheumatoid Arthritis (RA), Fibromyalgia (FMS), and Sarcoidosis inflammation. It
appears that the hidden locations of the suspected RA and FMS bacterial
inflammation generators have at last been recognized and made visible.
Pleomorphic (shape-changing) microbe elements (1/10th to 1/100th
the size of the blood-borne forms of the bacteria) have been identified in
colonies inside the cytoplasm of more types of blood cells. Pictures of the
macrophage intracellular colonies related to Sarcoidosis are found at: www.sarcinfo.com/remission.htm.
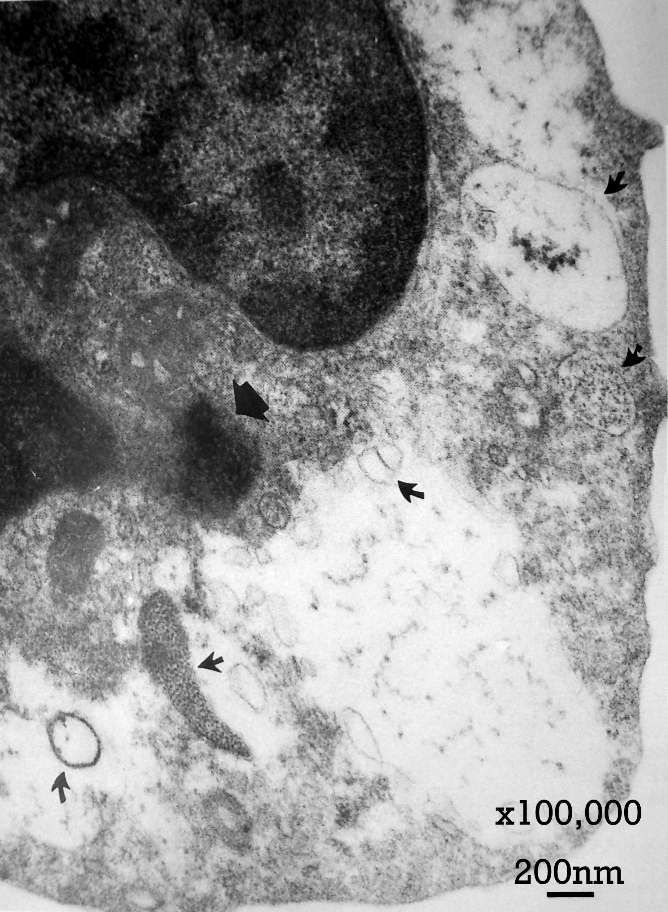
Dr. Trevor Marshall states, “Emil and Barbara Wirostko produced stunning
electron microscope photographs of immune phagocytes each containing hundreds
of tiny bacterial forms, around 0.01 - 0.025 microns in diameter, living in
colonies within the very cells (phagocytes) which are supposed to kill these
bacterial parasites.” One Wirostko
photograph.
This invasive
capability is well known in viruses, bacteria, certain yeasts (fungal forms)
and even larger microbes like the more complex Malaria parasite, Plasmodium falciparum. The presence of these colonies is suggested
as the root cause of many (perhaps most) so-called chronic “autoimmune”
diseases of heretofore unconfirmed etiology. The colonies contain exogenous DNA
and RNA that codes the generation of pathogenic bioactive molecules such as
hormones, toxins and enzymes.
The colonies of macrophages manufacture vitamin D (1,25-D), resulting in a surplus which poisons and can paralyze muscles, which have a D3 receptor for it. Excess blood concentration of the active form of 1,25-D has shown to be linked to inflammation in Sarcoidosis, Chronic Fatigue Syndrome, Lyme Disease, FMS and other autoimmune illnesses. [Reference: J. C. Waterhouse, Ph.D. ]
The D-ratio is the concentration in the blood of the 1,25-D hormone form of vitamin D (picogram/ml) divided by the concentration of the 25-D inactive, precursor-molecule form (nanogram/ml). If the D-ratio is greater than 1.3, this indicates an abnormal equilibrium excess of the active hormone. This excess is strongly correlated to both the presence of latent, intracellular (macrophage) parasite Cell Wall Deficient (CWD) bacteria and to the associated TH1 cytokine, so called “autoimmune cascade”. The 1,25-D stimulates hematopoietic conversion of stem cells into new macrophages, which become targets for colonization. Dr. Marshall shows a Table of Sarcoidosis patients’ D-ratios versus the 1,25-D concentration
Jarisch-Herxheimer
reaction and the inflammation cascade:
In severely
colonized patients, attacking the parasites may trigger severe Jarisch-Herxheimer (JH) reactions. Suppressing
vitamin D and minimizing sunlight exposure may be beneficial in moderating the
inflammation cascade. Vitamin D supplements may accentuate so called “allergic”
reactions.
Angiotensin II blockers also have beneficial effects in mediating JH attacks by blocking the production of inflammatory T1 cytokines, especially TNF-alpha. In Sarcoidosis, the offending metabolite is most likely 1,25-(OH)2-D and the synthetic source is the disease-activating macrophage. About 50% of hypercalcemic patients with lymphoma harbor frankly elevated or inappropriately high serum 1,25-(OH)2-D concentrations. [Reference: Marshall TG, Fenter B, Marshall FE: Putative Antibacterial Mechanisms for Angiotensin II Receptor Blockers. JOIMR 2004;2(2):1]
Angiotensin receptor blockers (ARBs) have wider applicability moderating other types of inflammation in addition to the heart related inflammation. However, blocking the inflammation cascade without eliminating its source, the latent bacterial colonies will not have any long-term effectiveness. [Reference: Adams JS: Vitamin D metabolite-mediated hypercalcemia. Endocrinol Metab Clin North Am. 1989 Sep;18(3):765-78.]
According to Dr Marshall’s: (Complete Text)
“The two hormones critical to this inflammatory process are Angiotensin II and the seco-steroid 1,25-dihydroxyvitamin-D.
“We use the Angiotensin Receptor Blocker 'Olmesartan Medoxomil' (Benicar/Olmetec/Votum), dosed approximately every 6 hours, to blockade the Angiotensin II receptors in the inflamed tissue.
“The seco-steroid 1,25-D is the active hormone resulting from sunlight on our skin, and the Vitamin D we ingest. Both these sources of 1,25-D have to be attenuated if these bacteria are to be killed.
“Blockade of Angiotensin II weakens these bacteria to the point where they can be more easily killed, and reducing the 1,25-D makes it harder for the bacteria to slip in and out of the cells they have infected.”
The enzyme
hyaluronidase plays a part in the invasion, acting as a penetrating factor in
dissolving the cell wall by unlinking the hyaluronate part of the cell wall or
membranes. Vitamin C acts to disable the hyaluronidase enzyme, to some degree
protecting the target cells. Dr. Aristo Vojdani (ImmunoSciences Lab) has found a daily ascorbic
acid intake of > 5 g/day to have normalized leukocyte production, where
levels were depressed. Other studies have
demonstrated “an antioxidant-induced increase in macrophage phagocytosis. Ascorbate depletion results in an impaired mitogen response
and reduction in IL-2 production, which is restored with vitamin C repletion.”
Classic tetracycline antibiotic treatment is phase II of the three-phase Marshall Protocol: Parts of the Marshall Protocol are similar to the combined anti-inflammation plus tetracycline treatment advocated first by Dr. Thomas McPherson Brown in The Road Back (1988). An updated Minocycline protocol for RA and FMS is also described in Appendix II of Rheumatoid Arthritis: The Infection Connection. This protocol is an effective long term slow-recovery treatment to suppress the intracellular parasites.
Phase I of the Marshall Protocol includes a combination of Benicar (an angiotensin II receptor blocker, or ARB), vitamin D avoidance/control, sunlight avoidance, shielding the eyes from bright light, weaning from prednisone and hydrocortisone, quercetin for anti-inflammation, and especially initial cessation of DMARDS (Sulfasalazine, Plaquenil, Methotrexate, antibacterials, anti-malarials, quinolones, Erythromycin, etc.)
Later, long term, low dosage antibiotic (Minocycline is preferred over Doxycycline), administered with a short 48 hour periodicity, ~25 mg dosage along with the continued Benicar used to control the cytokine cascade related to the continuing Jarisch-Herxheimer reactions. Probiotics and acidophilus supplements will act against yeast and dysbiosis. Minocycline dosage is gradually increased to higher levels to act against the correspondingly reduced concentration of these bacteria, their L-forms, and their colonies.
Still later, other antibiotics are introduced to target specific residual microbes that may remain. Phase II and III protocols are available to medical professionals. QA forums are actively moderated.
Vitamin C (>5 gm/day/180#) blocks the hyaluronidase enzyme spreading factor of bacteria, viruses, and tumors because C helps to block cellular invasion, leading to intracellular colonization, especially by Streptococcus pneumonia, Chlamydia pneumoniae, Mycoplasma penetrans, etc. Vitamin C has an effect of increasing phagocyte production, which in Phase I of the Marshall Protocol may not be the desired effect. However, later, if macrophage invasion can be effectively blocked, phagocytes at normal levels can be beneficial.
Dr. Marshall links excess vitamin D with muscle paralysis due to the D3 receptor in skeletal muscle. [Reference 1: Ashizawa, et al, “Hypertension due to vitamin F intoxication with clinical features mimicking acute myocardial infarction” and Reference 2: Bischoff, et al, “In situ detection of 1,25-dihydroxyvitamin D3 receptor in human skeletal muscle tissue.”] Both citations note the paralysis effect of excessive hormone vitamin D form on muscles.
(References 1 and 2 above are from the cited Bibliography in the article by Marshall TG and Marshall FE: The Science Points to Angiotensin II and 1,25-dihydroxyvitamin D. JOIMR 2003;1(2):3.)
One wonders if this possibly infection-localized effect is the cause of the relaxation of muscles which support adjacent joints, spine, etc., and the feeling of fatigue in those muscle areas. Work needs to be done to determine the D-ratio when these symptoms are communicated, especially in the case of spondylitis, spinal stenosis, CFS, FMS, and osteoarthritis.
Return to RA-Infection-Connection Home Page
{kind=link}
{kind=link}